

Selling into a clinic is not a smaller version of selling into a hospital. It is a different sale with a different buyer, a different clock, and a different reason for saying no.
Teams from enterprise healthcare arrive expecting procurement, security review, and a committee. Teams from general B2B arrive expecting a fast, simple close because the business is small. Both are wrong, and both waste a quarter finding out.
Learning how to sell to clinics means learning to sell to an owner-operator: a person who can approve your contract this afternoon and who has roughly four uninterrupted minutes to hear about it. No procurement department is protecting them. Nobody's job is to evaluate you either.
Why clinics are a different buyer than hospitals
Private practices, independent physician groups, med spas, and specialty clinics share a structure that changes everything about the sale.
- The owner is a clinician. The person with signing authority is usually seeing patients all day. Their decision-making time is whatever is left over.
- There is no procurement. No RFP, no vendor questionnaire, no six-month evaluation. That sounds like good news until you realize there is also no defined process for you to enter.
- The cycle is short but fragile. Decisions can happen in weeks. They can also evaporate in one busy week because nobody was assigned to move it forward.
- Every dollar is visible. A hospital line item disappears into a departmental budget. A clinic owner feels the cost personally, because it often is personal.
- Attention is the scarcest resource in the building. Not budget. Not interest. Attention.
- Staff turnover breaks continuity. The office manager who loved your product in March may not be there in June, and nobody will tell you.
If your target is a health system rather than an independent practice, the mechanics are entirely different and are covered separately in the hospital and health system go-to-market playbook. This article stays with the owner-operator, because running a committee-shaped sales process at a four-provider practice is a reliable way to be ignored.
Who actually decides in a private practice
The organization chart is small. The politics are not.
- Owner / managing physician - What they control: Final approval and the money. What they need from you: A short, credible reason this makes the practice better off.
- Practice manager - What they control: Access, priorities, vendor relationships. What they need from you: Confidence you will not create work or embarrassment.
- Office manager / front desk lead - What they control: Daily execution and adoption. What they need from you: Proof their day gets easier, not harder.
- Lead physician (in groups) - What they control: Clinical veto and peer influence. What they need from you: Assurance that care quality is not compromised.
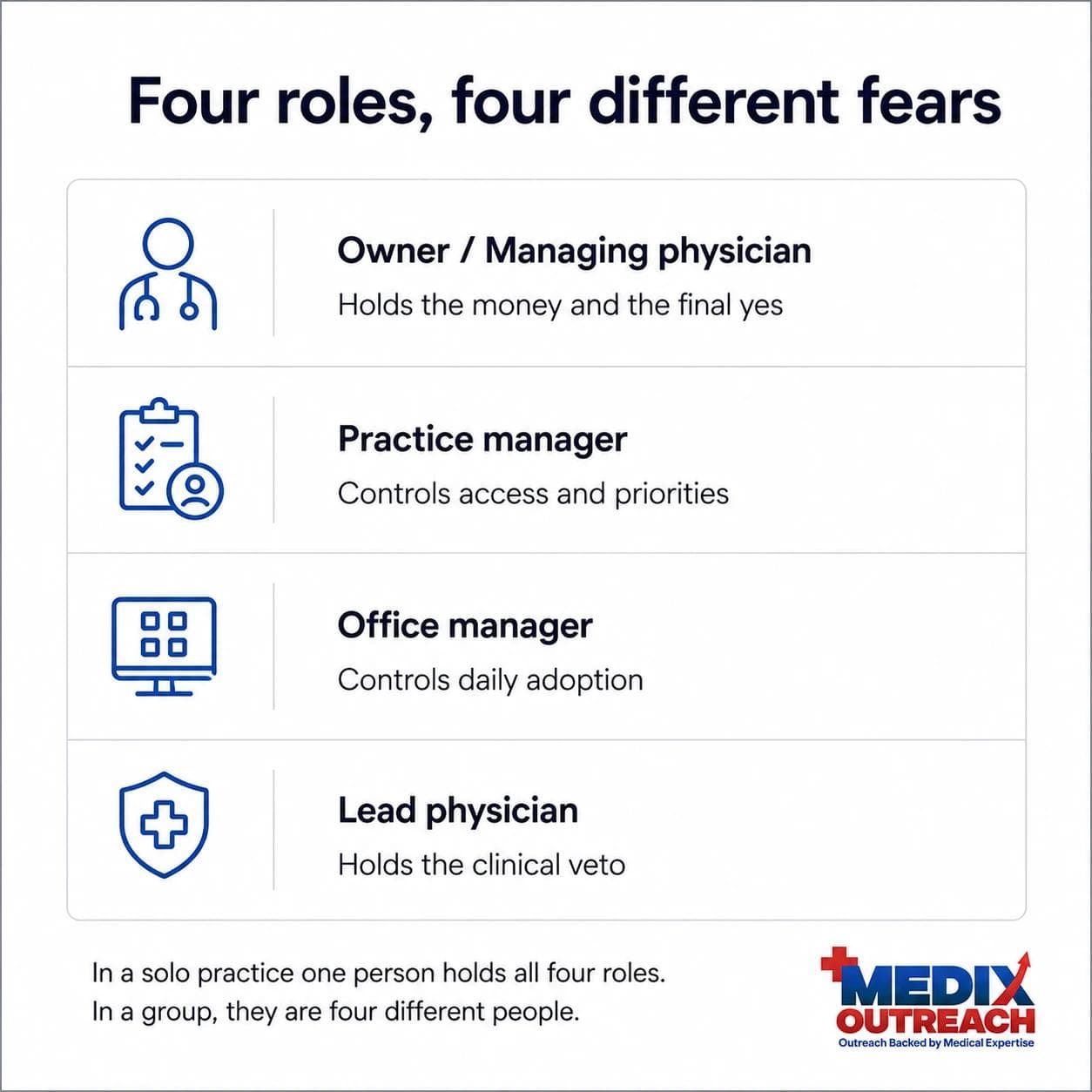
In a solo practice, one or two people hold all four roles. In a ten-provider group, they are four different humans with four different fears. Selling to independent physicians means knowing which version you are in before the first call, not after the third.
The practice manager is the real first contact
Most vendors try to reach the doctor. That instinct is understandable and usually wrong.
The practice manager is not an obstacle standing between you and the buyer. In most practices, they are the person who decides whether the owner ever hears your name. They know the budget, the pain points, the vendors who burned them, and what the owner has already said no to twice.
Treat that role as the primary audience for the first conversation, not as a switchboard. The vendors who get through show up with something the practice manager can use, rather than a request to be passed along.
That shift is what changed the outcome in the Be Seen Health provider positioning work, where refining the practice-manager conversation and removing financial risk from the offer did more than any change to the product itself.
What clinics actually buy
Healthcare providers rarely adopt technology because it is innovative. They adopt solutions that reduce administrative burden, improve patient outcomes, support reimbursement, enhance workflow efficiency, or increase practice revenue.
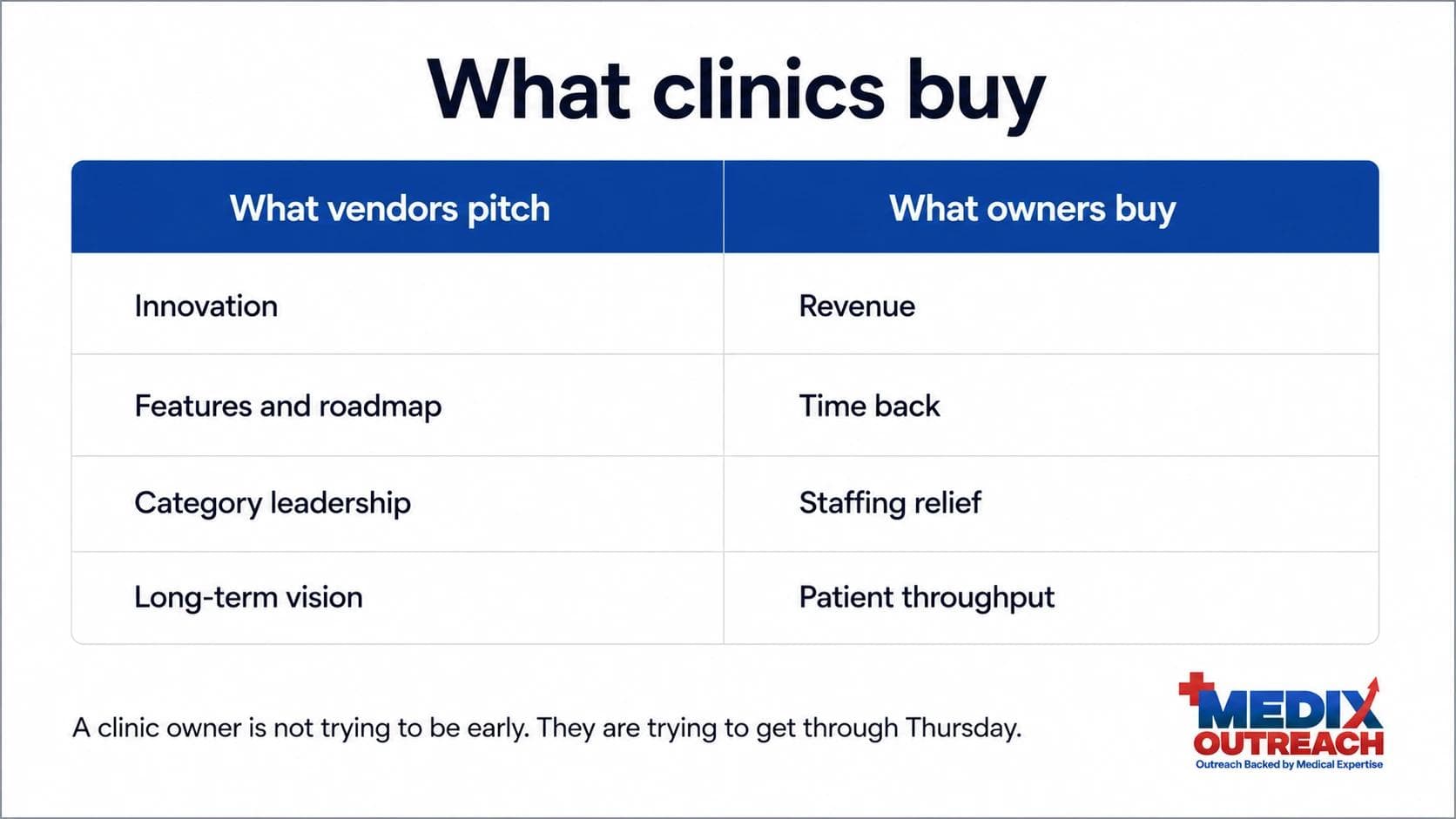
In a clinic, that list compresses even further. There are four things an owner-operator will reliably spend money on.
- Revenue. More visits, better payer mix, a new service line, fewer no-shows, faster collection.
- Time. Anything that gives clinicians back part of their day. Time is the currency they are shortest on and never budgeted for.
- Staffing relief. If your product means the practice avoids a hire, or that the person they cannot replace stops quitting, you are selling something urgent.
- Patient throughput. Same rooms, same staff, more patients seen without a drop in care quality.
Notice what is missing. Innovation is not on the list. Neither is a feature comparison, a roadmap, or a category. A clinic owner is not trying to be early. They are trying to get through Thursday.
That gap is the underlying reason most cold outreach fails in healthcare. The message is about the product. The buyer is thinking about their week.
How to reach practice managers and clinic owners
Clinics are reachable in a way health systems are not. A human answers the phone. A person reads the general inbox. That access is an advantage, provided you respect how the building runs.
Timing is a real variable, not a detail
A clinic has a rhythm. Mornings are the intake crush. Midday is charting and callbacks. Late afternoon is a race to close out. Monday is triage from the weekend. Friday afternoon is nobody's decision window.
Calling into the busiest hour does not just fail. It teaches the person on the phone that you do not understand their world, and that impression is expensive to undo. Ask a practice manager when the quiet window is and they will tell you. Very few vendors ask.
The phone still works here
In small practices, a well-timed call is often faster and more respectful than a fourth email. The bar is preparation: know the practice, know the specialty, and have a reason to call that is about them. The case for that channel is laid out in why cold calling still earns conversations in healthcare.
Email has to be specific or it is noise
Generic outreach does not work in healthcare. A clinic inbox is full of vendors, and the filter the reader applies is simple: does this person know anything about my practice, or is this a template?
Specificity means naming the specialty, the workflow, and the pressure. "Practices like yours" is not specific. "Most HRT clinics we work with are losing revenue at the refill hand-off" is. The rules for making healthcare email land are covered in healthcare email that gets read rather than filtered.
Mid-article CTA
Need help building your healthcare growth engine?
Medix helps healthcare startups, clinics, pharma companies, and provider-focused platforms build scalable commercial pipelines.
Book a Strategy CallThe clinic sales cycle
The clinic sales cycle is short in calendar terms and shallow in stages, but it stalls in predictable places. It usually looks like this.
- Contact. You reach the practice manager, not the owner. Goal: earn ten minutes, not a demo.
- Qualification. Establish whether the pain is real, funded, and owned. If nobody in the building is personally annoyed by the problem, there is no deal here yet.
- Owner conversation. Short, direct, economic. This is where revenue, time, staffing, and throughput get named in the owner's own numbers.
- Trial or pilot. Small, bounded, and defined by what success looks like before it starts.
- Commitment. Fast once the owner is convinced, because there is nobody left to consult.
- Onboarding. The stage most vendors treat as administrative and the stage where clinic deals actually die. If the front desk cannot use it in week one, it is already churning.

The most common failure is not rejection. It is silence after a good meeting, because the deal had a champion but no owner, or an owner but no next step. Nothing moves in a clinic unless someone in the building has a reason to move it this week.
Pricing and risk reversal for a buyer who fears being locked in
Clinic owners have been sold to before, usually badly. Most have signed a twelve-month agreement for something that was never used, and that memory shapes every pricing conversation you will have.
So the objection is rarely the price itself. It is the exposure. What happens if this does not work and I am still paying for it in eight months?
Structures that reduce that fear tend to move deals faster than a discount:
- Short initial terms or a defined pilot period.
- Pricing tied to activity or outcome rather than a flat commitment.
- No charge for things outside the practice's control, such as no-shows.
- No upfront fee where the model allows it.
- A clear, plainly worded exit. Ambiguity reads as a trap.
Discounting an unchanged structure signals that the original price was arbitrary. Removing the downside signals confidence. Owner-operators respond to the second.
Common mistakes when selling to medical practices
- Running a hospital process at a clinic. Multi-stakeholder decks exhaust a buyer who wanted a straight answer.
- Bypassing the practice manager. This is remembered, and it is remembered by the person who controls access.
- Leading with the product. The clinic does not want your category. They want Thursday to be easier.
- Ignoring the clock on the wall. Contacting a clinic during the morning rush is a self-inflicted wound.
- Selling to the enthusiast. A friendly office manager is not authority. Find the owner or accept the deal is not real.
- Asking for a long commitment first. The buyer's fear is entrapment, not cost.
- Treating onboarding as done. Adoption failure in week one is the quiet cause of most clinic churn.
Where a pharmacist-led approach changes the clinic conversation
Great healthcare products still fail without the right market access. In the clinic segment, that gap is almost always a translation problem: the vendor speaks product, the practice speaks operations, and neither side is wrong.
A pharmacist-led approach starts inside the care setting rather than outside it. Knowing how a practice runs, what the staff are protecting, and which objections are real rather than polite exits changes what gets said and who gets contacted first. It also changes what does not get said, which matters more than most founders expect.
That is the structure behind Medix Outreach's provider network development work, which follows a Research, Engage, Activate, Manage sequence rather than starting with campaigns. Healthcare innovation does not scale until providers believe in it, and belief is built one practice at a time. Building that footprint across independent clinics nationally is the work behind the Atomix Research clinic pipeline.
The background behind that approach sits on the About Medix Outreach page, alongside the full set of healthcare growth and business development services.
Frequently asked questions
How do you sell to clinics without a procurement process to follow?
You supply the process yourself. With no vendor evaluation path in place, the seller has to provide the structure: a clear first conversation, a bounded pilot, defined success measures, and an explicit next step at every stage. Left alone, a clinic deal stalls because nobody owns the next move, not because a decision was made.
Who is the decision maker in a private practice?
The owner or managing physician holds final authority in most independent practices. The practice manager usually controls whether the owner ever hears about you, and the office manager controls whether the product survives after signature. All three matter, and they matter at different stages.
How long is the clinic sales cycle?
Considerably shorter than a health system cycle, and highly variable. Small practices can decide in weeks once the owner engages. The unpredictability comes less from the decision itself and more from how long it takes to get a busy owner's attention.
Is cold calling still effective when selling to medical practices?
It can be, more so than in enterprise healthcare, because a human answers the phone. Effectiveness depends on timing and preparation. A prepared call in the quiet window respects the practice. An unprepared call in the morning rush does lasting damage.
What is the biggest mistake vendors make with independent physicians?
Selling innovation instead of relief. Independent physicians run a business under time pressure. A pitch built around technology or novelty asks them to do translation work they have no time for.
How should we price for clinics that fear being locked in?
Reduce the downside before you reduce the price. Short terms, pilot periods, activity-based pricing, and a clearly worded exit address the real objection, which is exposure rather than cost.
How can Medix help with selling into clinics?
Medix Outreach helps healthcare companies identify the right practices, build positioning that matters to an owner-operator, run the outreach that reaches practice managers, and manage the relationships after activation. The approach is healthcare-native and pharmacist-led. You can start with a strategy call.
Final thoughts
Knowing how to sell to clinics comes down to accepting what kind of buyer you are dealing with. Not a committee. Not an enterprise. A clinician running a business with no spare attention, no procurement cover, and a memory of the last vendor who wasted their time.
The vendors who win here are rarely the ones with the best product. They are the ones who show up prepared, at the right hour, with a specific reason to talk and an offer that does not feel like a trap.