

Most practices that want more referrals treat the problem as a marketing problem. It is not. It is a relationship problem with a workflow attached.
A referral is one physician handing another physician their patient and a piece of their reputation. That is a business-to-business decision made under clinical risk. It has little in common with a patient choosing a clinic from a search result, and tactics do not transfer between the two.
This guide is about earning referrals from other providers, not about advertising to patients. What follows is the provider-to-provider side: why referrals stall, what a referring doctor needs from you, and how to build a referral engine that keeps producing.
Why physician referrals stall
When referral volume flattens, the explanation is rarely that the referring physician forgot you. It is that referring to you costs them something. Understanding how to get more physician referrals starts with naming that cost. A referring provider is exposed three ways every time they send a patient out the door.
- Their patient carries the risk. A long wait, a rushed visit, or a bad experience lands on the person who made the referral.
- Their reputation is the collateral. The referral is an endorsement. A bad outcome reflects on their judgment, not only on you.
- Their continuity is at stake. A patient who never returns, or returns confused about who manages what, is a case they are still accountable for.
A referral is therefore a small act of trust with an asymmetric downside, which is why volume is far more sensitive to friction and silence than to friendliness. It is also why cold, generic approaches struggle. The dynamics that cause cold outreach to fail in healthcare apply with more force when the ask is not a meeting but a patient.
What a referring provider actually needs
Ask a primary care physician why they favor one specialist over another. The answers are boringly consistent, and never about marketing.
Fast, predictable access
Access is the most decisive factor in most referral relationships. A referring provider is standing in a room with a patient who needs to be seen. If you can see that patient in a timeframe matching the clinical urgency, you are useful. If your first available is three months out and nobody says so, you are a liability. Predictability matters as much as speed: an office that knows you can absorb an urgent case this week, and knows how, will use you again.
Closed-loop communication back
This is where most referral relationships die, and it is almost always fixable. The referring physician sent the patient. Then nothing. No note, no plan, no indication of what is managed by whom. Closing the loop means the referring provider gets back, reliably and quickly:
- Confirmation the patient was contacted and scheduled, or a flag that they were not.
- A concise note with the assessment and plan, written to be read in under a minute.
- A clear statement of what you are managing and what stays with them.
- A heads-up when something changes materially.
None of that is a courtesy. It is the product. A specialist who closes the loop is easier to refer to than one who is marginally better clinically and silent.
Confidence the patient comes back
Any suspicion that a referral is a one-way transfer rather than a shared episode of care ends the relationship without a conversation. The specialist who reliably hands the patient back, with a clear plan, gets more referrals than the one who absorbs them. State it explicitly.
Map who to build relationships with
The instinct is to introduce yourself to every physician within driving distance. That produces a long list of people who vaguely know your name and a short list who actually refer. A referral network is built, not collected. Start by narrowing.
- Start with your existing referrers. Pull twelve months of referrals by source. A small group usually produces most of your volume, and your fastest growth is inside it.
- Identify who should be referring and is not. Practices in your catchment, in the right specialty mix, who send you nothing. Each is a question: do they not know you, or did something go wrong?
- Look past the physician. Coordinators, practice managers, and medical assistants often decide where a referral goes. The physician says "send them to a dermatologist." Someone else picks which one.
- Segment by clinical overlap. Group sources by why they would send you a patient, not by size.
Ten PCP relationships that each send two patients a month beat a hundred introductions that produce nothing. This kind of mapping drove the work behind provider positioning for clinic adoption, where practice-manager conversations mattered as much as physician conversations.
The referral workflow is the product
The easiest practice to refer to wins a disproportionate share of referrals, and "easy" is a design decision. Walk your own referral pathway as if you were a referring office.
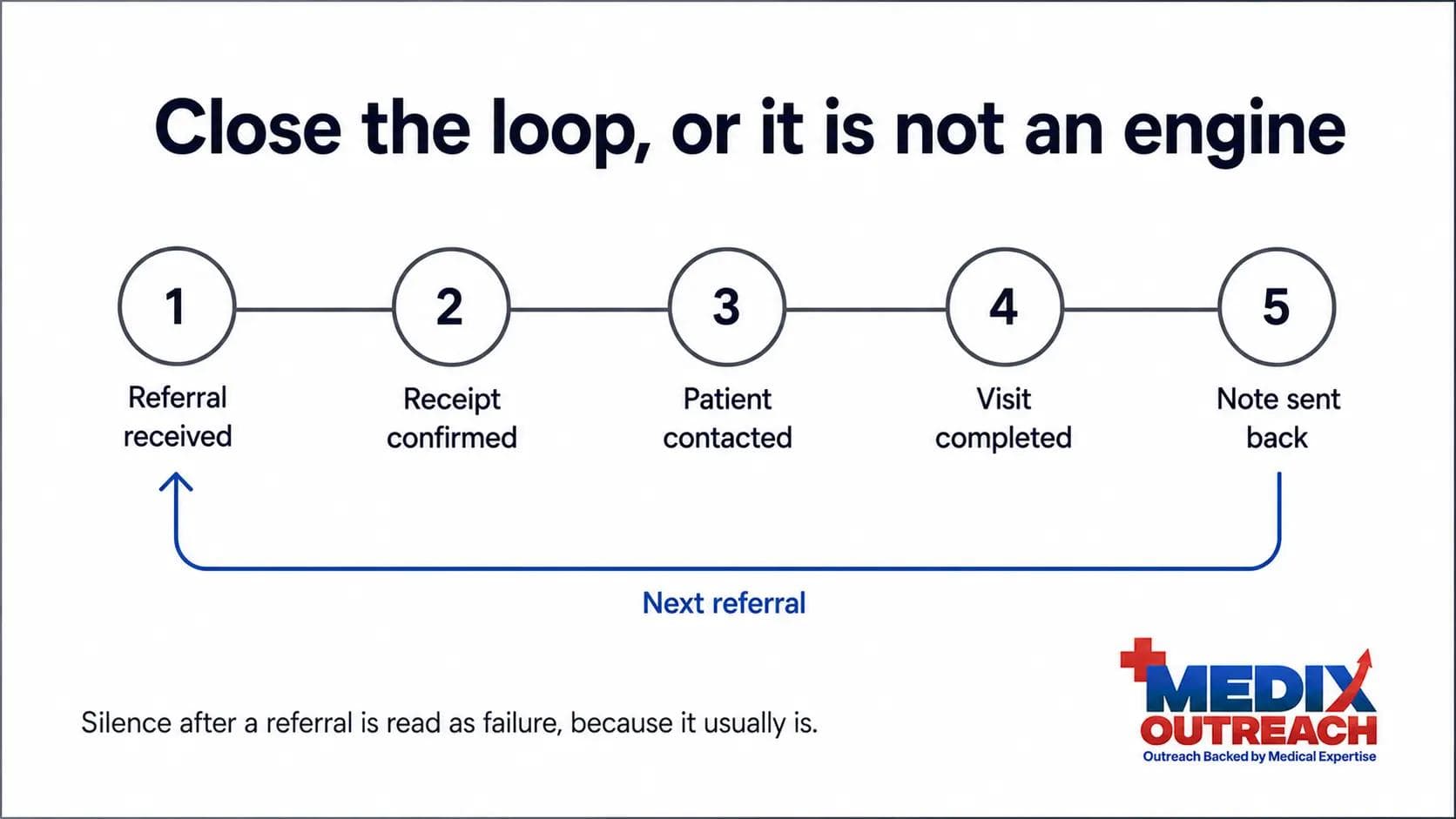
- How does a referral reach you? One obvious route, or does every office guess?
- Who owns it in the first 24 hours? A named person, or a queue?
- Does anyone confirm receipt? Silence after a referral is read as failure, because it usually is.
- How fast is the patient contacted? Not scheduled. Contacted. The referring office starts the clock when they hit send.
- What goes back, and when? If the answer is "eventually, if someone remembers," you do not have a referral engine.
- When the patient never books, does the referring office find out?
Fix the pathway before you invest in relationships. Building referral volume that your intake then drops damages your reputation with the exact people you wanted to impress. Referral workflow, physician partnership development, and the CRM automation behind both sit inside patient acquisition and practice growth for this reason. The relationship and the operation are one system.
Clinical education as outreach
The way to become the obvious referral choice is not to be memorable. It is to be useful. Clinical education outreach does that work: a lunch-and-learn on a treatment pathway, a case discussion on when to refer versus when to manage. It does three things at once:
- It demonstrates competence rather than asserting it. Thirty minutes of clinical substance tells a PCP more about your judgment than any brochure.
- It clarifies the referral criteria. Most under-referral is not resistance. It is uncertainty about what you treat and when you want to see the patient.
- It puts you in the room with the whole team. The coordinators and MAs who route referrals are usually there, and frequently the deciding vote.
Most agencies build campaigns. Healthcare relationships are built on clinical credibility, earned where you are the one contributing something. An anonymized psychiatry practice built exactly this motion - PCP partnerships, a defined referral workflow, and lunch-and-learn education - in the psychiatry provider referral engine case study. A similar pattern shows up in local provider partnership work around prescription fulfillment, built on solving an operational problem rather than on being visible.
Mid-article CTA
Need help building your healthcare growth engine?
Medix helps healthcare startups, clinics, pharma companies, and provider-focused platforms build scalable commercial pipelines.
Book a Strategy CallWhy "thank you notes and cookies" advice fails
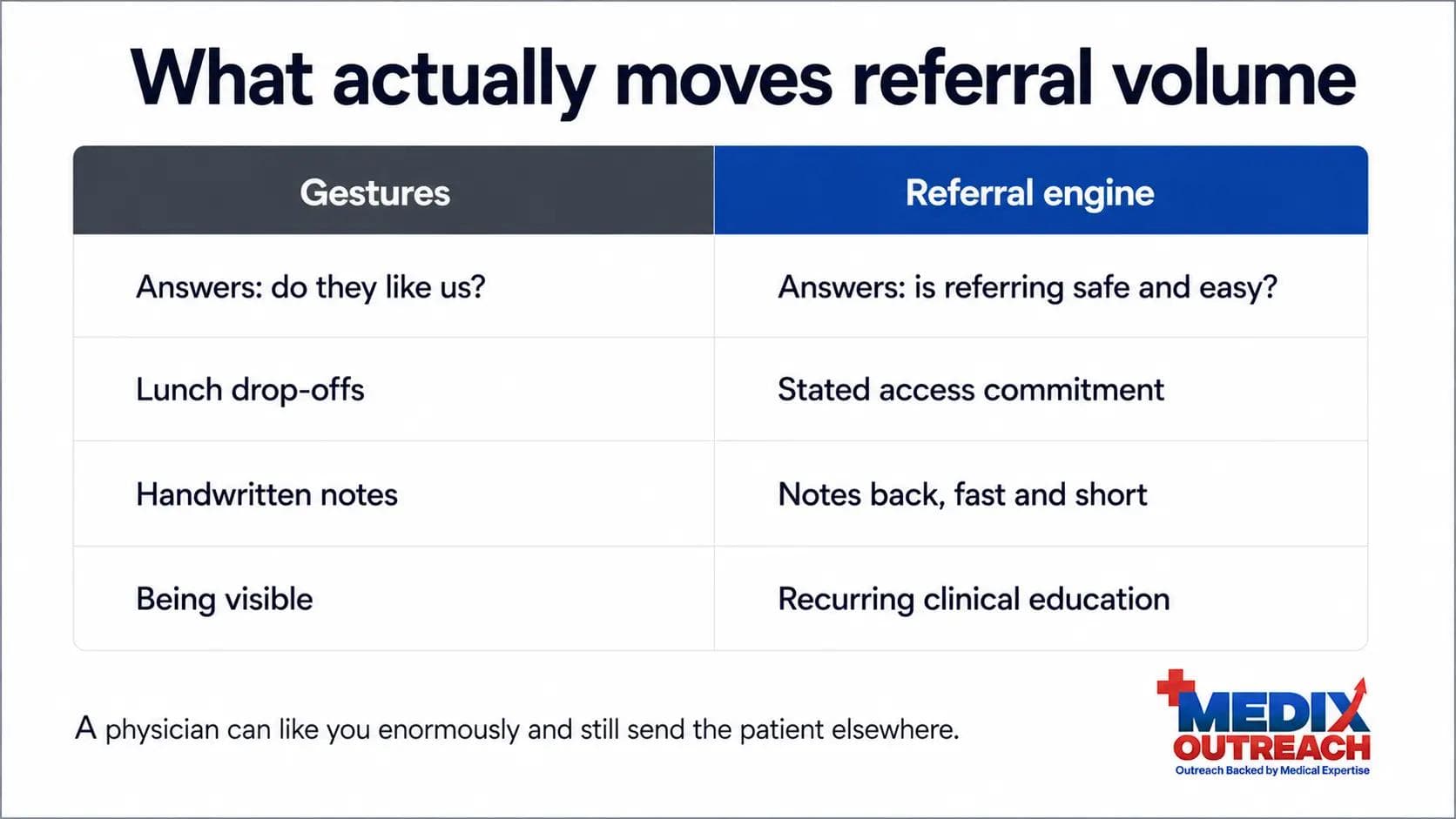
Search for referral advice and you will find the same suggestions: drop off lunch, send handwritten notes, be visible, build rapport. None of it is wrong. It is just downstream of everything that matters. Gestures address whether the referring physician likes you. Referrals are decided by whether referring to you is safe and easy. A physician can like you enormously and still send the patient to whoever answers first.
There is also a boundary worth being deliberate about. Physician referral relationships in the United States sit near Stark Law and the Anti-Kickback Statute, and anything resembling giving items of value in exchange for referrals is a serious matter, not a growth tactic. This article is not legal advice. Build your program around access, communication, and clinical education, and have counsel review it.
The replacement for gestures is unglamorous:
- A named contact a referring office can reach.
- A stated access commitment you keep, including a route for urgent cases.
- Notes that go back fast and read fast.
- Recurring clinical education instead of episodic visibility.
- A standing feedback channel, so problems surface as complaints instead of silence.
Relationships still matter, and direct conversation is often the right move. There is a real case for calling in healthcare business development. The conversation just has to be backed by an operation that delivers.
Measuring referral growth
Most practices measure total referral volume and have no idea why it moved. An engine needs metrics that point at a cause.
- Referrals by source, by month. The base layer. Without it, everything else is anecdote.
- Active referrer count. Distinct sources that sent a patient this quarter. The honest measure of network breadth.
- New versus reactivated sources. New and lapsed relationships are different problems with different fixes.
- Referral-to-appointment conversion. Leakage here is an intake problem, not a relationship problem.
- Time to first contact. Hours from referral received to patient reached. This quietly determines whether you get the next one.
- Loop closure rate. Share of referrals where a note went back within your target window.
- Source concentration. Volume share from your top three referrers. High concentration is a growth ceiling and a risk.
Review by source, not in aggregate. A referrer going quiet has a specific cause, recoverable if you notice within weeks rather than a year.
Common mistakes when building a referral network
- Treating referrals as marketing. Patient-facing tactics run at physicians read as noise.
- Building relationships on top of broken intake. More referrals into a leaky pathway produces more disappointed referrers.
- One-time introductions. A single visit builds recognition, not habit.
- Never asking what went wrong. Referrers do not complain. They just stop.
- Chasing new sources while existing ones decay. Reactivating a lapsed referrer is usually the cheapest volume available.
- Sending marketing material instead of clinical substance. A brochure asks for something. A case discussion gives something.
Where a pharmacist-led approach helps
Referral development fails most often on translation. The practice knows its clinical value. The people building the outreach do not speak the language of the offices they approach, so the message lands as promotion instead of a peer conversation.
A pharmacist-led team starts from inside healthcare. Understanding physician workflows, provider objections, reimbursement conversations, and referral dynamics changes what gets said in a lunch-and-learn, which practices get approached first, and which operational fix comes first. Generic outreach does not work in healthcare, least of all when the ask is a patient. That perspective is the basis of the work at Medix Outreach, a pharmacist-led consultancy, and it runs through the wider set of healthcare growth and business development services. The broader provider-marketing motion, of which referral development is one part, is covered in the guide to marketing to doctors.
Frequently asked questions
How do you get more physician referrals?
Make referring to you low-risk and low-effort: fast, predictable access, a pathway with a named owner and a confirmation step, notes that go back quickly, and recurring clinical education with the practices you want referrals from. Volume follows reliability.
Is physician referral marketing the same as patient marketing?
No. Patient marketing addresses a consumer choosing a provider. Referral development is a B2B relationship between clinicians, driven by clinical risk, access, and communication. The channels, message, and measurement all differ.
How long does it take to increase physician referrals?
It depends on the starting point. Fixing intake and closing the communication loop can move volume from existing referrers quickly, because those relationships already exist. Building new ones takes longer, since referral behavior forms through repeated positive experience rather than a single meeting.
Who should we build referral relationships with first?
Start with the referrers you already have, especially those who have gone quiet. Then move to practices with the right clinical overlap in your catchment that send you nothing. Include coordinators and practice managers, since they frequently decide where a referral goes.
Do lunch-and-learns actually work?
They work when they are clinical education rather than a sales visit. A session that clarifies referral criteria or walks a treatment pathway gives the team something useful and demonstrates your judgment. A pitch with food attached does not.
Are there compliance considerations with physician referrals?
Yes. Referral relationships in the United States are subject to laws including Stark Law and the Anti-Kickback Statute, and the rules around anything of value connected to referrals are strict. This article is general education, not legal advice. Have qualified healthcare counsel review any referral program first.
How can Medix help build a referral engine?
Medix Outreach helps specialty practices and provider-facing companies map referral sources, tighten the referral workflow, develop physician partnerships, and run clinical education that earns referrals rather than asking for them. The approach is pharmacist-led. You can start with a strategy call.
Final thoughts
Referral growth is not a campaign. It is an operating standard: answer fast, see the patient, close the loop, hand them back, and show up with something worth their time.
Practices that do this look unremarkable from the outside. They are simply the easiest and safest option in their market, and referring physicians choose easy and safe.