

There is a specific kind of quiet that settles over a healthtech company several months into its first serious pilot. The product is live. The clinicians are happy. The weekly call is friendly. And nothing is happening.
This is pilot purgatory: proof of interest, proof of usage, sometimes proof of value, and no revenue. The board sees logos. The bank account sees nothing.
The move from a digital health pilot to contract is where most healthtech commercial plans quietly break - not because the software failed, but because the pilot was never designed to end in a decision. This guide covers why, what to settle before you agree to a pilot, and what to do when one is already drifting.
Pilot purgatory is a commercial design failure, not a product failure
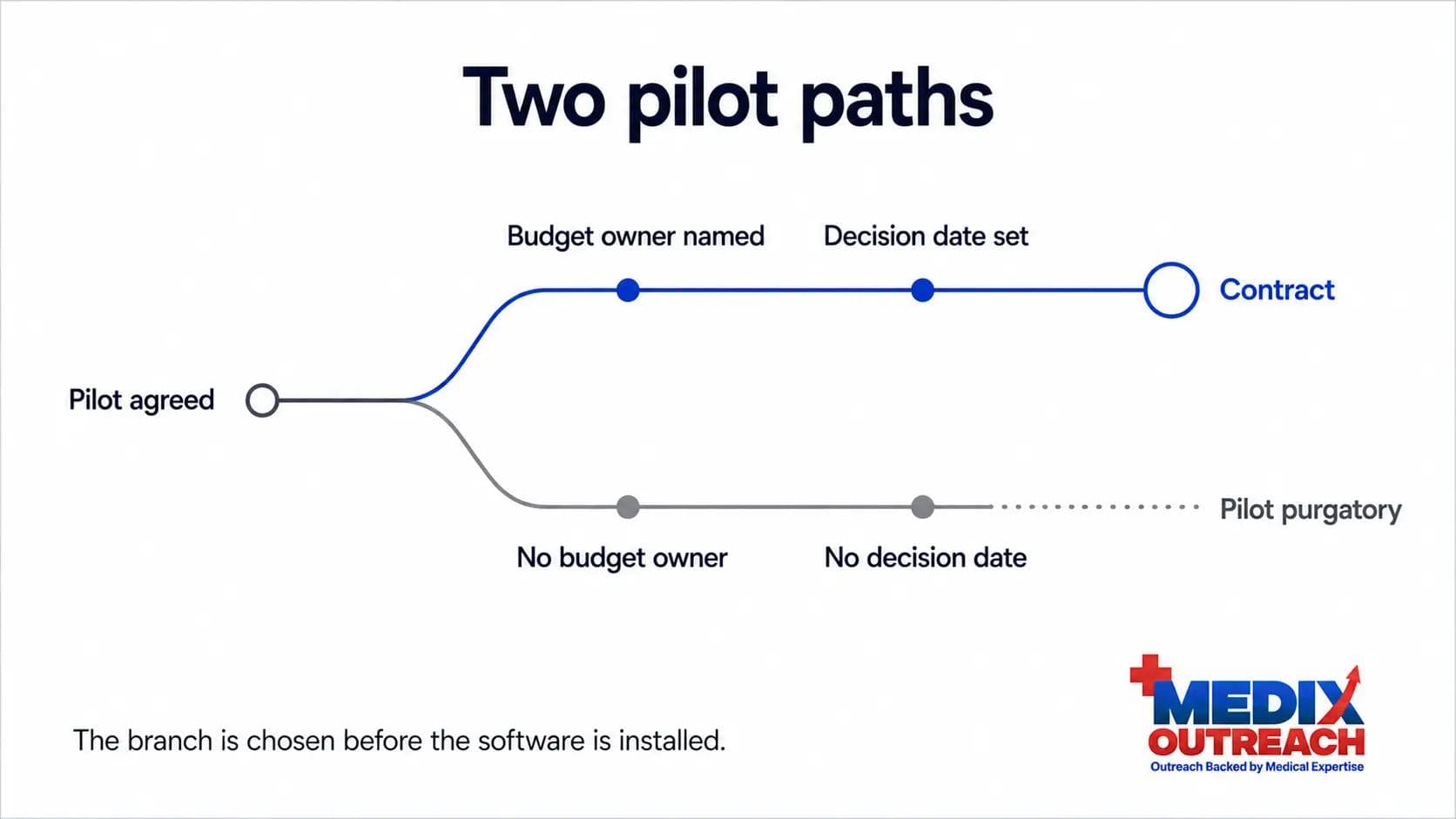
Founders almost always diagnose a stalled pilot as a product problem. The reasoning is intuitive: if they loved it, they would buy it. So the team ships more features and waits. But a pilot stalls because of things decided, or left undecided, before the software was installed:
- Nobody agreed what result would trigger a purchase.
- No budget was ever identified for the version of this that is not free.
- The person who championed the pilot cannot authorize the contract, and never could.
- No date forces a decision, so there is always a better week to make it.
- The measure being tracked is the vendor's metric, not something the organization is judged on.
Every item on that list is a commercial design choice. The outcome is controllable, and the fix belongs at the front of the process, not the back.
Why health systems love pilots, and why that is the trap
From a health system's perspective, a pilot is close to a perfect instrument.
- It costs almost nothing. No capital request, no committee, no procurement cycle.
- It carries no commitment. Nothing has to be renewed or defended if it fades away.
- It looks like progress. Innovation teams are often measured on activity, and a pilot is activity.
- It buys optionality. The system watches a category mature without picking a vendor.
- It ends quietly. Nobody has to say no. It just stops being mentioned.
So a fast yes may be the cheapest available way to say "not now." This is the mechanism behind what founders call death by pilot: not hostility, just an institution behaving rationally with a free option. An unstructured pilot is not a sales stage. It is a parking space, and an eager vendor pays for the parking.
A note on where this sits: the buying committee, the security review, and everything on the way into a health system is covered in our playbook for selling to hospitals, which ends where a pilot is agreed. This article picks up there.
Settle these five questions before you agree to a pilot
The highest-leverage moment in the pilot lifecycle is the conversation before you say yes. Once it is running, your leverage only falls, because you have given away the thing they wanted. Five questions need real answers, not optimistic ones.
- Who owns the budget if this succeeds? Name the person and the budget line. If the sponsor is an innovation group with no operating budget, you are running a pilot into a room with no door.
- What result makes this a yes? A specific threshold on a specific measure, written down.
- When is the decision made? A date. Then work backwards: if the decision lands in Q3 but the budget cycle closes in Q2, your real deadline is earlier than the one you were given.
- Who signs? Rarely the champion. Meet them during the pilot, not after it.
- What happens if it works? Ask them to describe the next step in their own words. If they cannot, it does not exist yet, and your job is to help them build it.
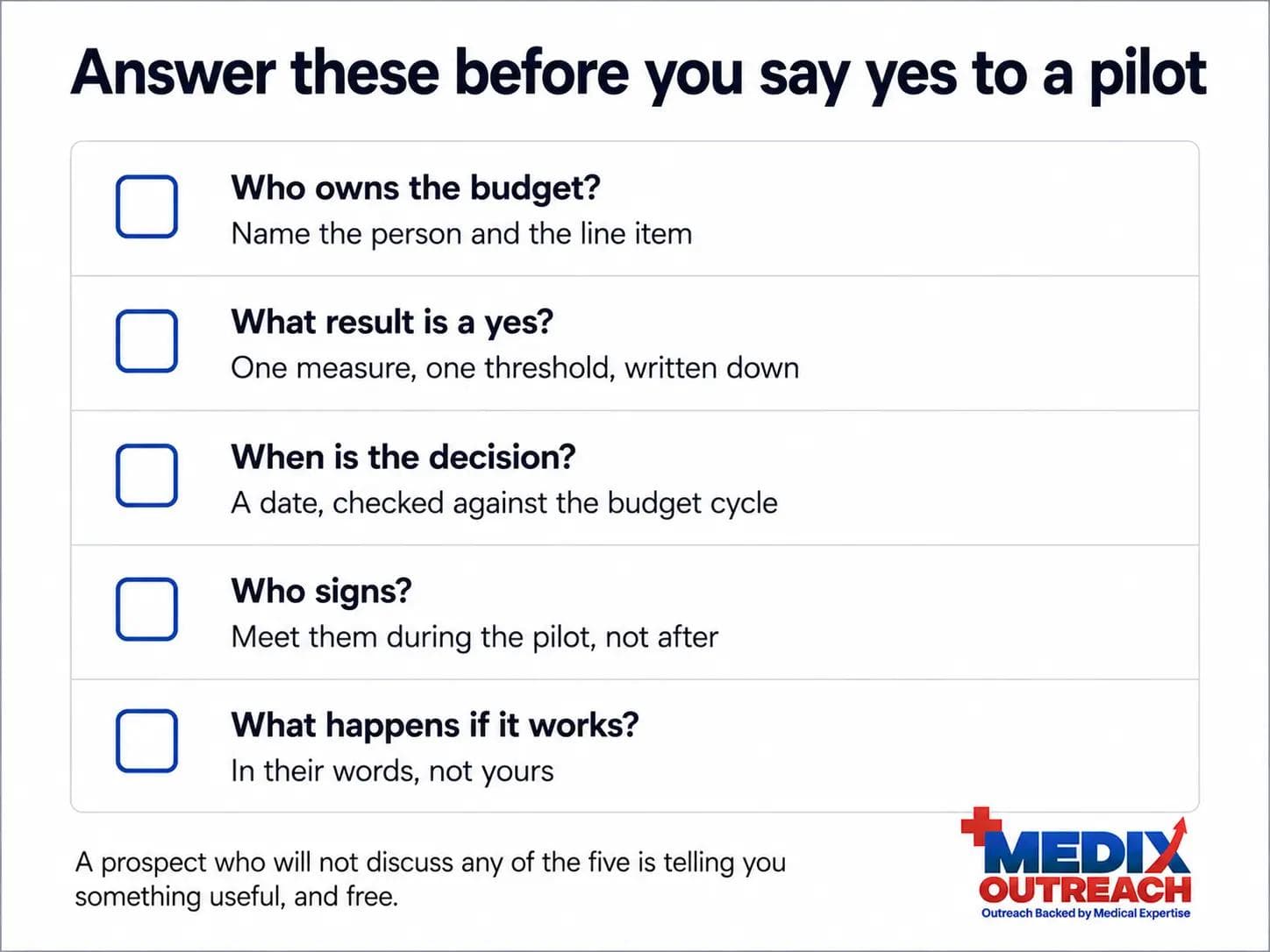
Asking these does not lose deals. It loses pilots that were never going to convert, which is the point.
Free pilots versus paid pilots
The instinct to give the pilot away is understandable, especially for a first logo. It is also the decision that most reliably produces purgatory.
A free pilot has no internal owner. Nobody had to defend it, so nobody is exposed if it dies. Money creates accountability - not because the amount matters, but because someone signed something and now wants a result. Charging also shifts the internal question from "should we buy this?" to "should we keep this?" The second is easier to win.
Free can still be right - for a design partner shaping the roadmap, or a reference customer in a segment you need. What makes those legitimate is trading the fee for something specific: an executive sponsor, a written decision date, agreed criteria, and access to the signer. A pilot with no fee and no commitments is not a pilot. It is a donation.
Keep this framing commercial. Anything that becomes contractual language should be drafted by your counsel.
Design success criteria the buyer already cares about
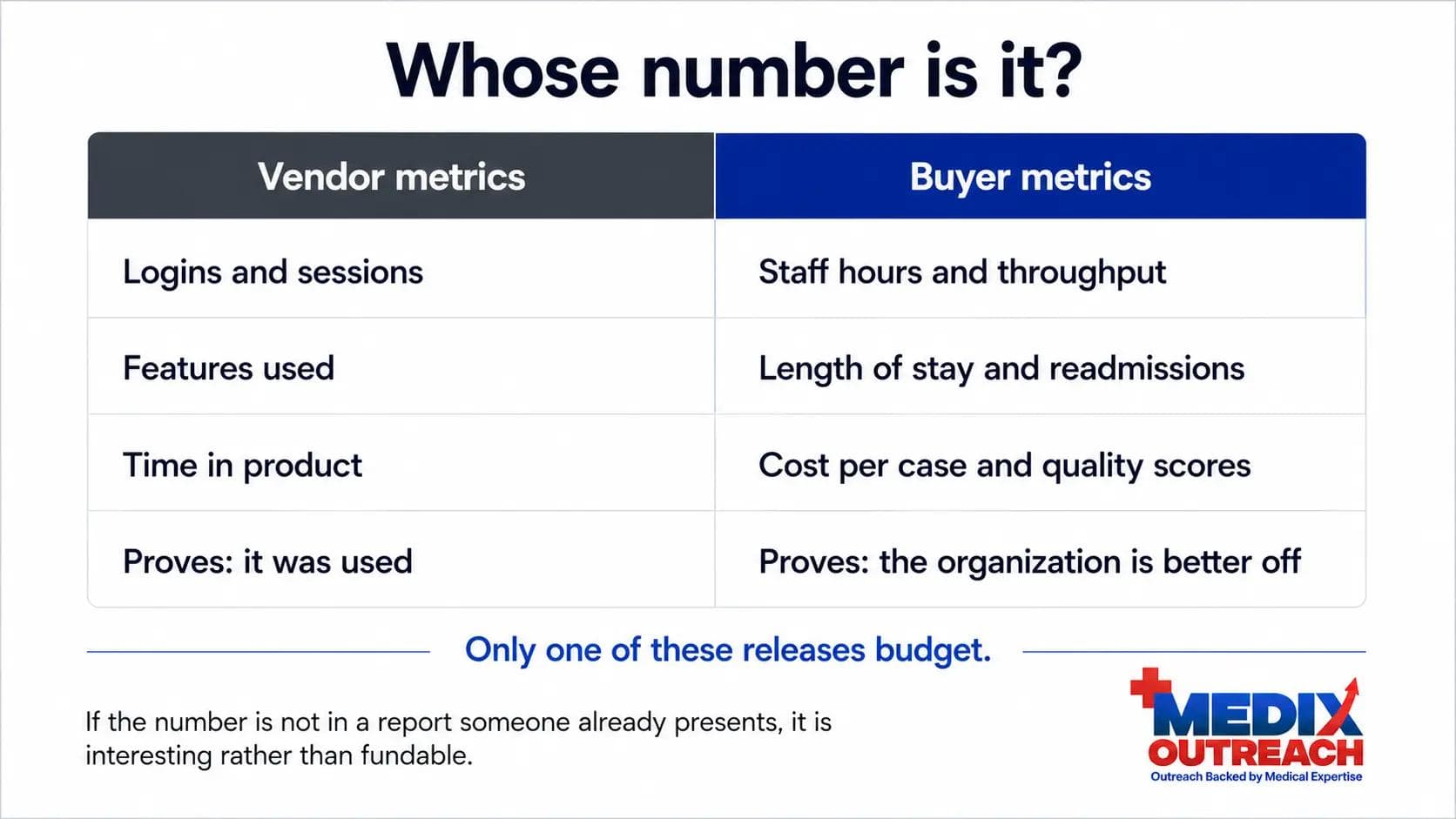
Most pilot success criteria are written by the vendor, and it shows. They measure what the product does, in units the vendor finds flattering. But the buyer is not evaluated on your metric. They are evaluated on theirs.
The test: does this number appear in a report someone there already has to present? If not, your result is interesting rather than actionable, and interesting does not get funded.
Vendor metrics look like usage, logins, and time in product. Buyer metrics look like readmissions, length of stay, staff hours, throughput, cost per case, and quality scores. The first set proves your product is used. The second proves the organization is better off.
Three rules follow:
- Pick one primary measure, not six. With six, the one that underperforms becomes the story.
- Agree the baseline before you start. Anything arguable gets argued.
- Set a threshold you can clear. A pilot that "improved things" produces a debate. One that cleared a number the buyer chose produces a decision.
Who defines those measures matters too, which is the broader argument in our piece on clinical credibility as a commercial asset.
Mid-article CTA
Need help building your healthcare growth engine?
Medix helps healthcare startups, clinics, pharma companies, and provider-focused platforms build scalable commercial pipelines.
Book a Strategy CallThe champion problem
Champions move. People change jobs everywhere, but healthcare deals take long enough that the odds of yours still holding that seat at decision time are worse than in most industries. Long cycles are covered in our look at why healthcare sales cycles keep stretching.
When a single-threaded champion leaves, the pilot rarely gets cancelled. It gets orphaned, which is worse, because nothing forces a conclusion. The successor inherits a project they did not choose, with a vendor they did not pick.
What protects against this:
- Multi-thread deliberately. Build real relationships across three roles: the clinical user, the operational owner, and the budget holder.
- Keep a written record the organization owns. A shared summary of scope, criteria, baseline, and dates that survives any individual leaving.
- Make the champion's job easy. They argue your case in rooms you are not in. Give them one page they can forward unedited.
- Watch the signals. Meetings pushed twice, the champion delegating downward, phrases like "next fiscal year." That is the pilot dying, not scheduling noise.
Build the expansion path into the pilot itself
A pilot should not end with a question. It should end with a step that was already agreed.
That means the conversation about what comes next happens at the start, while the buyer is enthusiastic and unpressured, rather than at the end, when it sounds like a sales push. Align on the shape of the scaled deployment before the pilot begins: which departments or sites come next, roughly what the commercial model looks like at that scale, and what has to be true for it to proceed. You are not asking for a commitment. You are asking them to imagine the future in enough detail that the pilot becomes a step toward it.
This is where the framework Medix uses for healthcare commercial growth and go-to-market work - Discover, Position, Activate, Scale - does more than describe a sales process. Scale is not a phase that starts once the pilot succeeds. It is one you design during Position, or it never arrives.
What to do when a pilot is already stalling
Most teams reading this do not have a clean slate. They have live pilots and a board meeting. The recovery sequence is short.
- Get honest about the stage. A pilot with no budget owner and no decision date is not a late-stage deal. Reforecast it before someone else does it for you.
- Ask the five questions now. Frame it as planning the next phase properly, not as chasing.
- Propose a formal conclusion. Offer a readout with the champion, the operational owner, and the budget holder, on a date. A pilot without an ending never has a decision.
- Force a real answer. Give the buyer permission to say no. "If this isn't a priority this year, that's useful for us to know" converts more pilots than any follow-up sequence, because it removes the comfort of drifting.
- Fix the intake, not just this deal. If two pilots stalled for the same structural reason, the problem is qualification, not luck - the core of building a first B2B healthcare sales funnel that holds up.
Common mistakes on the way from pilot to contract
- Treating a signed pilot as a won deal. It is permission to prove something, not a purchase.
- Running the pilot with the enthusiast only. Enthusiasm is not authority, and it does not survive a personnel change.
- Measuring what your product does instead of what they are judged on. Usage data does not release budget.
- Letting the pilot run long. Extensions feel like momentum. They are usually an unmade decision wearing a friendly face.
- Saying yes to every pilot. Three unqualified pilots cost more attention than a lost deal.
- Leaving commercials until the end. A first pricing conversation after the results is a second sales cycle from scratch.
Where a pharmacist-led perspective helps
The gap that produces pilot purgatory is usually a translation gap. The founding team understands the technology. The health system understands its own operating pressure. The pilot gets designed in the space between.
A pharmacist-led approach starts inside the care environment rather than outside it. It changes which metric gets proposed, which stakeholder is brought in during week two rather than month six, and which objections get answered before they are raised. It also changes what does not get promised, which matters with an audience that has watched vendors overreach.
In one engagement with a US-based clinical decision support platform, structured outreach led to six pilot evaluations initiated inside health systems alongside 28 qualified commercial meetings. Getting to the pilot is its own discipline. The pilot is where the commercial work starts.
You can read more on the Medix Outreach team page, or see the full range of healthcare business development services.
Frequently asked questions
What is pilot purgatory?
Pilot purgatory is the state where a digital health company has live pilots, engaged users, and no paid contracts. The pilots do not fail and they do not convert. They persist, producing logos instead of revenue.
Why do healthcare pilots fail to convert into contracts?
Usually because the pilot was structured without the things that force a decision: a named budget owner, an agreed threshold on a metric the buyer cares about, a decision date, and access to the signer. Without those, nothing makes the organization choose.
Should a digital health pilot be free or paid?
Paid is generally better, because a fee creates an internal owner who needs a result. Free can make sense with genuine design partners, but only if you trade the fee for named commitments: a sponsor, agreed criteria, a decision date, and access to the signer.
How long should a health system pilot run?
Long enough to produce a defensible result on the agreed measure, and no longer. The length is set by the metric and the baseline, not the calendar. Extensions usually signal an unmade decision, not a need for more data.
What should pilot success criteria measure?
Something the buyer is already accountable for. If the number does not appear in a report someone there has to present, it will not release budget. Agree one measure, a baseline, and a threshold before the pilot starts.
How can Medix help move a digital health pilot to contract?
Medix Outreach helps healthtech teams structure pilots commercially: qualifying which to accept, identifying the budget owner, shaping criteria the buyer recognizes, and building the expansion path in from the start. The approach is healthcare-native and pharmacist-led. You can start with a strategy call.
Final thoughts
The pilot is not a milestone. It is a mechanism, and mechanisms only produce what they were built to produce.
A pilot designed to demonstrate a product will demonstrate a product, indefinitely, at your expense. A pilot designed to force a decision will produce one - sometimes a no you can act on, sometimes a contract. The difference is not the software. It is the conversation you had before you said yes.