

Most healthcare SaaS companies do not have a product problem. They have a go-to-market problem that looks like a product problem.
The software works. Early users like it. But the pipeline is thin, deals stall in places the team did not plan for, and the outreach that worked at a previous SaaS company produces silence here. The instinct is to build more features. The actual issue is that the go-to-market motion was designed for a buyer who does not exist in healthcare.
A healthcare SaaS go-to-market strategy has to account for a buyer who is clinically trained, time-poor, risk-averse, and rarely acting alone. This guide covers how to choose a segment you can win, how to position against the things providers actually care about, how to plan for the buying committee, and how to sequence a launch so that evidence arrives before it is demanded.
Why healthcare SaaS go-to-market is different
Standard SaaS go-to-market assumes a few things that do not hold in healthcare: that a motivated user can buy, that value is self-evident in a trial, and that speed is a competitive advantage.
- The user is often not the buyer. A physician can love your product and still have no budget, no authority, and no appetite for the internal fight required to get it approved.
- Adoption is a clinical risk decision. Anything touching patient care, documentation, or prescribing gets weighed for safety before it is weighed for convenience.
- Workflow is the real competitor. Your product is not competing with another vendor. It is competing with the way the clinic already does it, which is free and familiar.
- Integration is a gate, not a feature. EHR compatibility, data security, and IT review can stop an approved decision cold.
- Trials do not sell themselves. A busy clinician will not explore your software to discover value. If the value is not obvious in the first session, the trial quietly dies.
- Timelines are long enough to kill startups. Budget calendars and committee schedules do not compress because you raised a round.
None of this makes healthcare unwinnable. It means the go-to-market has to be built for a slower, more collective, more evidence-driven decision than the one most SaaS playbooks assume.
Choose a segment narrow enough to actually win
The single most common healthcare SaaS go-to-market mistake is a segment defined so broadly that no message can be written for it.
"Providers" is not a segment. "Clinics" is not a segment. A segment is specific enough that you can name the workflow, the pressure, and the person who feels it. Independent dermatology practices with three to eight providers who are losing time to prior authorizations is a segment. Health systems is not.
Narrow beats broad early for reasons that compound:
- You can write outreach that names their exact workflow, which is the difference between a reply and a delete.
- Your reference customers look like your next prospects, so proof transfers instead of evaporating.
- Word travels inside specialties. Clinicians talk to peers in their own field far more than across fields.
- Your product roadmap stops being pulled apart by contradictory requests from unrelated buyers.
What a healthcare ICP needs to include
A healthcare ideal customer profile needs more than firmographics. The attributes that predict whether a deal closes are usually operational and clinical.
- Setting and ownership. Independent practice, group, hospital-employed, private-equity-backed, and health system all buy differently.
- Specialty. This drives vocabulary, workflow, and which outcomes matter.
- Size. Provider count usually predicts whether there is a committee, a practice manager, or an owner who decides.
- The systems already in place. EHR and existing tooling determine integration effort and switching cost.
- The trigger. A staffing gap, a reimbursement change, a quality metric, or a growth target is what makes now different from last quarter.
- Who owns the budget. If you cannot name this role, you do not have an ICP yet.
If your team is building this foundation for the first time, it pairs closely with the work of setting up a first B2B healthcare sales funnel, where segment definition is what everything downstream depends on.
Position against burden and outcomes, not innovation
Healthcare buyers are not moved by novelty. They are moved by relief.
Providers adopt solutions that reduce administrative burden, improve patient outcomes, support reimbursement, fit the existing workflow, or improve practice economics. A product described as innovative, AI-powered, or transformative has told a clinician nothing they can act on. A product described as removing a specific step from a specific weekly task has told them everything.
A useful test: rewrite your homepage headline so it names a task the buyer did this week. If you cannot, the positioning is still about you.
Strong healthcare SaaS positioning usually holds four claims at once, and each one belongs to a different person in the decision.
- Clinical value - Who it convinces: Physicians, clinical leadership. What it has to answer: Does this improve care, or at least not compromise it?.
- Workflow value - Who it convinces: Nurses, staff, practice managers. What it has to answer: Does my day get easier or harder in week one?.
- Financial value - Who it convinces: Owners, finance, administrators. What it has to answer: What does this cost, protect, or return?.
- Implementation feasibility - Who it convinces: IT, operations. What it has to answer: What breaks, and who has to fix it?.
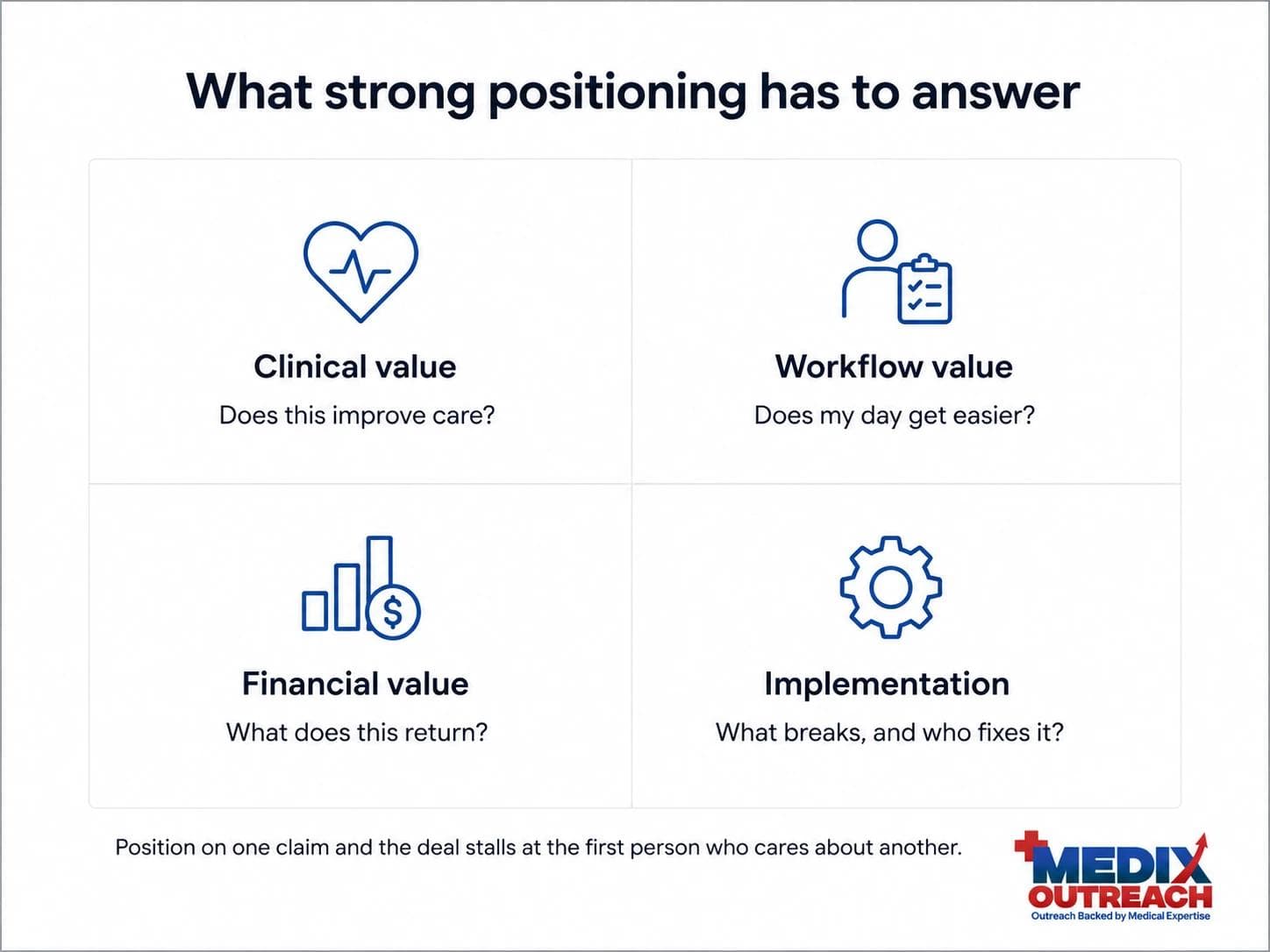
Position on only one of these and the deal slows at the first person who cares about a different one. This is the same discipline behind accelerating clinic adoption through strategic positioning, where competing on price against incumbents was replaced by a growth-enablement story the clinic could act on.
Plan for the buying committee before you build the funnel
Healthcare software decisions are collective, even in small practices. The size of the group scales with the size of the organization, but the group is almost never one person.
In a small independent practice, the group may be an owner, a practice manager, and whoever handles the EHR. In a health system, it can include clinical leadership, department heads, IT and security, procurement, finance, and compliance, each with a veto and none with a mandate to move fast.
Two implications change how you build the motion:
- Your champion is a messenger, not a buyer. The material you give them is what gets argued internally when you are not in the room. If your champion cannot explain your value in one sentence to a CFO, the deal is already stalling.
- Every added stakeholder adds a reason to say no. The job is not to excite everyone. It is to make sure no one has a defensible objection.
This is also why healthcare deals stretch. If the timeline is catching your team by surprise, the mechanics are covered in more depth in why healthcare sales cycles are getting longer.
Mid-article CTA
Need help building your healthcare growth engine?
Medix helps healthcare startups, clinics, pharma companies, and provider-focused platforms build scalable commercial pipelines.
Book a Strategy CallMatch the landing motion to the buyer
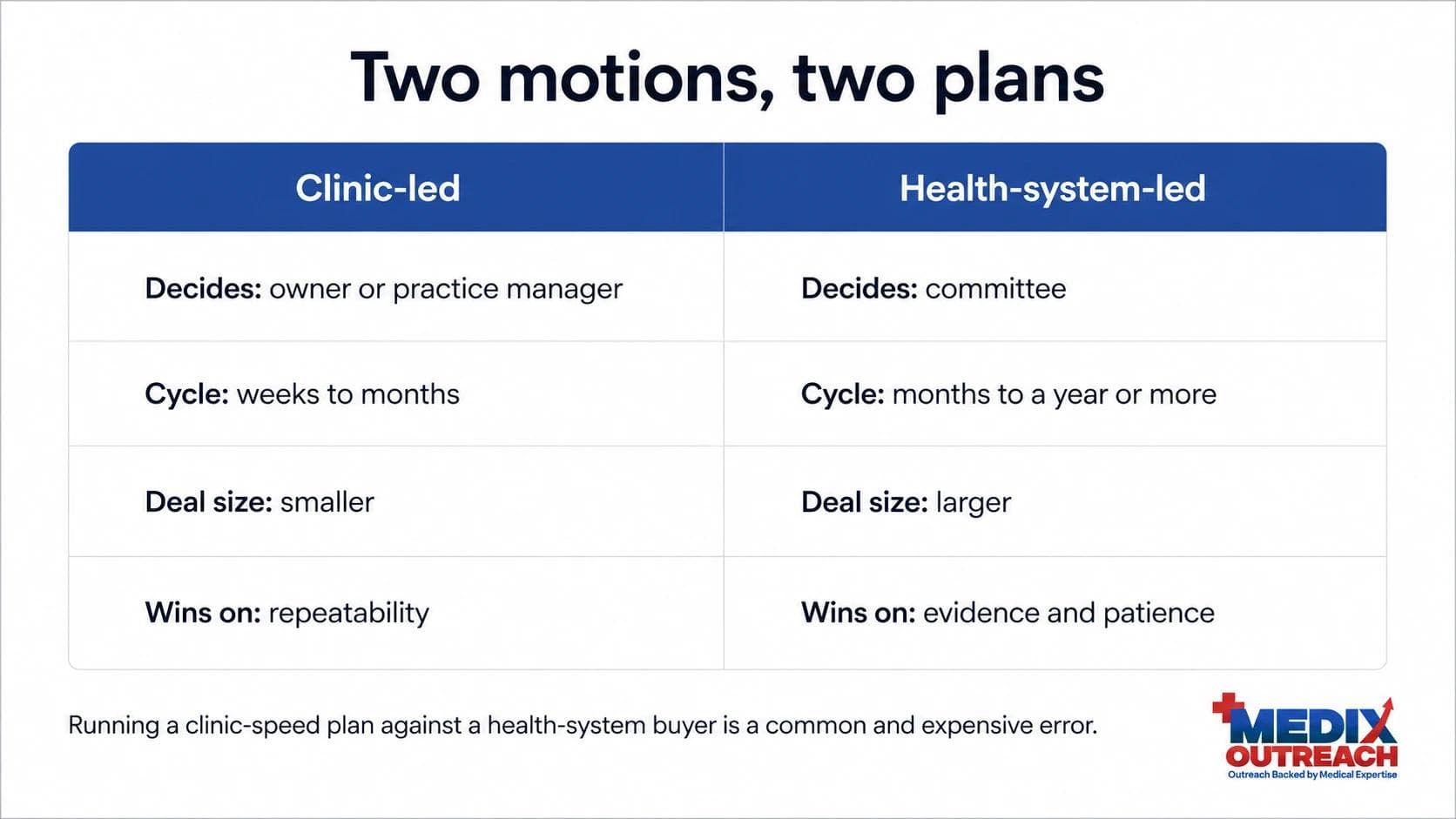
There is no single healthcare SaaS go-to-market motion. There are two common ones, and choosing the wrong one wastes a year.
The clinic-led motion
You sell to independent practices and small groups. The owner or practice manager can decide. Cycles run weeks to months. Volume matters, so the motion needs repeatability: accurate lists, specialty-specific messaging, and disciplined follow-up. The risk is that the deals are small, so the economics only work if acquisition stays efficient.
The health-system-led motion
You sell to hospitals and large systems. One deal is worth many clinic deals, but it takes committee review, security assessment, procurement, and usually a pilot. Cycles run many months to over a year. The risk is running out of runway before the first contract lands. The full mechanics of this path are covered in how to sell to hospitals.
Most teams should pick one deliberately and resource it properly, rather than running both badly. A common and expensive error is using a clinic-speed sales plan and cash flow forecast against a health-system buyer.
Build evidence before it is demanded
Healthcare buyers ask for proof at the exact moment you cannot manufacture it. Evidence is a go-to-market asset with a long lead time, which means it has to be planned during the launch, not after the first stall.
Evidence does not always mean a clinical trial. Depending on what you sell, credible proof can include:
- A structured pilot with success measures agreed in advance.
- Workflow data showing time saved or steps removed.
- A reference customer in the same specialty who will take a call.
- A clinician advisor who will speak to the clinical logic.
- A clear, conservative economic model the buyer can check.
The credibility of the person delivering the evidence matters as much as the evidence. That relationship between proof and trust is the subject of clinical credibility as a go-to-market asset.
Sequence the launch
A healthcare SaaS launch works better as four ordered stages than as parallel guesswork. Medix structures healthcare commercial growth and go-to-market work around the same sequence.
- Discover. Validate that the problem is real, expensive, and owned by someone specific. Talk to clinicians before writing messaging.
- Position. Build the claim set, the objection answers, and the one-sentence story your champion can repeat.
- Activate. Build accurate target lists, run role-specific outreach, and get into real conversations. Measure replies and meetings, not sends.
- Scale. Once a segment converts predictably, widen carefully into adjacent specialties or settings, keeping the proof transferable.
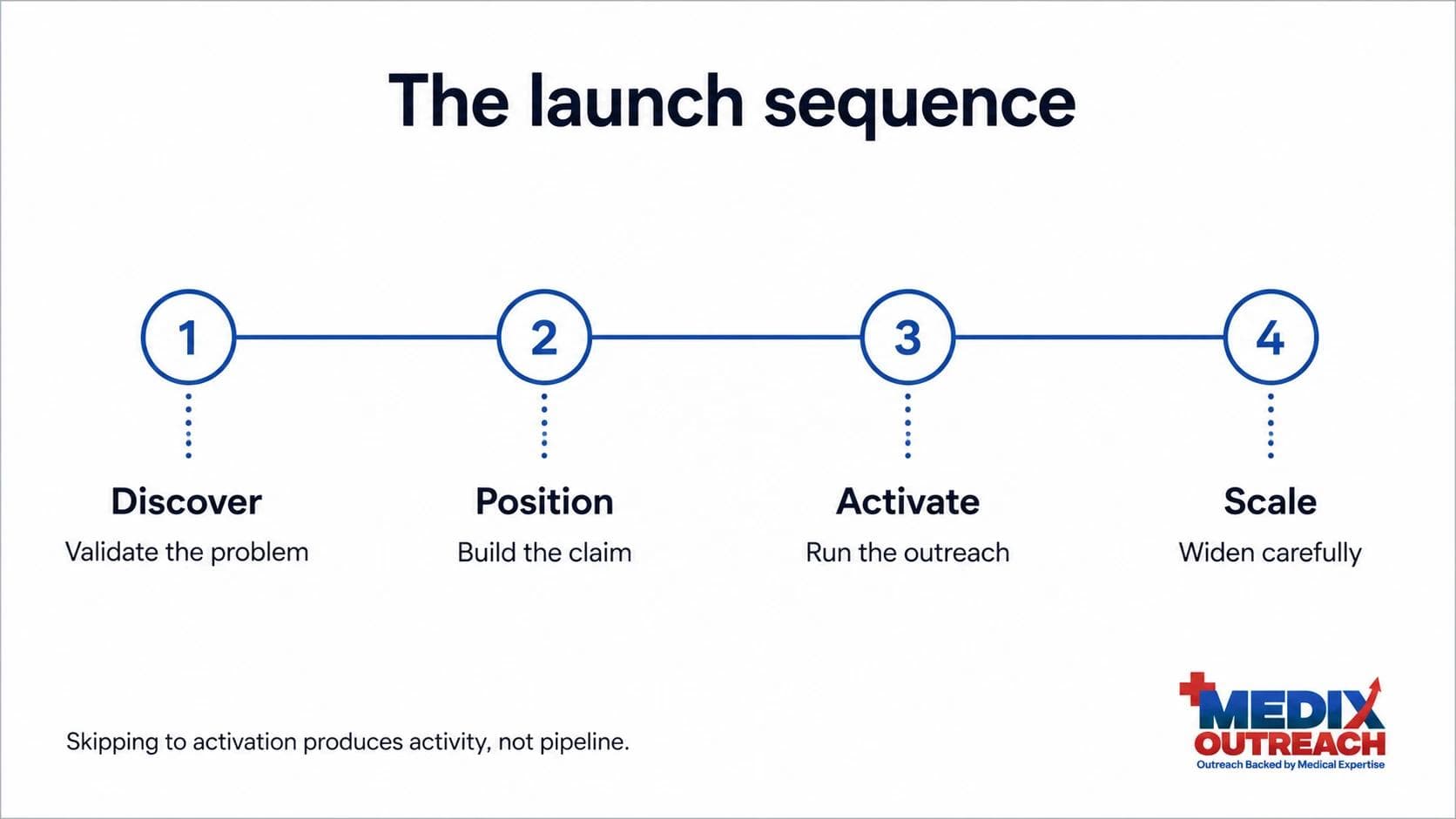
The failure mode is skipping straight to activation. Outreach built on unvalidated positioning generates activity, not pipeline, which is the core argument in why generic healthcare SaaS outbound is killing pipeline.
Common healthcare SaaS go-to-market mistakes
- Selling to "healthcare." A segment you cannot name in one sentence cannot be marketed to.
- Leading with technology. Innovation is not a benefit. Burden removed is a benefit.
- Assuming the enthusiastic user can buy. Enthusiasm is not authority.
- Ignoring the practice manager. In clinics, the gatekeeper often decides whether the doctor ever hears about you.
- Treating IT and security as paperwork. They are a gate, and they are usually the last people you meet and the first who can stop you.
- Planning cash flow on a SaaS timeline. Healthcare cycles are longer than the ones your board is benchmarking against.
- Waiting for the stall to build evidence. By then you are asking for time you no longer have.
Where a pharmacist-led approach changes the go-to-market
Most healthcare go-to-market problems come down to a translation gap. The team understands the software. The buyer understands the clinic. Nobody in the room speaks both.
A pharmacist-led approach helps because it starts inside the care world rather than outside it. Understanding formulary logic, prescribing behavior, provider objections, referral dynamics, and reimbursement conversations changes what gets written and who gets contacted first. It also changes what does not get said, which matters more than founders expect with a skeptical clinical audience.
This is the perspective Medix Outreach is built around, and it is why the work usually starts with segment and positioning rather than with campaigns. You can read more about that background on the About Medix Outreach page, or see the full range of healthcare growth and business development services.
Frequently asked questions
What is a healthcare SaaS go-to-market strategy?
It is the plan for who you sell to, what you say, how you reach them, and how a decision actually gets made. In healthcare it has to account for a clinical buyer, a buying committee, workflow risk, integration requirements, and a longer cycle than standard SaaS.
How is healthtech go-to-market different from normal SaaS?
The user often cannot buy, adoption is treated as a clinical risk decision, integration and security are gates rather than features, and trials do not sell themselves to a busy clinician. The result is a slower, more collective decision that rewards evidence and specificity over speed.
Should healthcare SaaS companies sell to clinics or health systems first?
It depends on the product and the runway. Clinics decide faster and are easier to reach, but the deals are smaller. Health systems are worth more but require committee review, procurement, and often a pilot. The mistake is running both motions at once with the resources for one.
How long does a healthcare SaaS sales cycle take?
It varies widely by buyer. Small independent practices can move in weeks to a few months. Health systems commonly take many months or longer, especially when the product touches patient care, data, or the EHR. Plan the pipeline and budget around the slower case.
What evidence do healthcare buyers expect?
Enough proof to defend the decision internally. That can be a structured pilot, workflow data, a same-specialty reference, a clinical advisor, or a conservative economic model. The exact form matters less than whether it is credible and easy for your champion to repeat.
How can Medix help with healthcare SaaS go-to-market?
Medix Outreach helps healthcare SaaS and healthtech teams define the segment, build the ICP, shape clinical and economic positioning, map the buying committee, and run the outreach motion that turns interest into qualified meetings. The approach is healthcare-native and pharmacist-led. You can start with a strategy call.
Final thoughts
A healthcare SaaS go-to-market strategy is mostly a set of decisions made before any outreach is sent: which segment, which claim, which motion, which proof, and in which order. Teams that make those decisions deliberately look patient and disciplined. Teams that skip them look busy.
The companies that win in healthcare software are rarely the ones with the most features. They are the ones whose story survives being retold by a champion to a committee that has never met them.